SPONDYLOS menu →








What is Adolescent Scoliosis?
Adolescent Scoliosis (scoliosis in teenagers) is when in a healthy adolescent between 9 and 13 begins the spine is rotating at different levels and opposite each other.
The rotation of the thoracic vertebrae and entrains the ribs leads to the formation of thoracic hump.

The same applies to the lumbar vertebrae where shall contribute the projection of the backmuscles to crate the hump.

It is the most common type of scoliosis (4 in 100 adolescents), affecting children aged 9 to 14 years. It evolves during the period of rapid growth.
Curves slow down their evolution during skeletal maturation. But all curves, without exception, continue to worsen in adulthood.
The progressive increase of the rotation of the vertebrae creates a lateral slope on the side of the turn like a twisted staircase.

What creates it?
The commonly used expression is Idiopathic Scoliosis that is of unknown etiology. The reasoning is rather well known. Gene etiology appears to be the most prevalent. It is due to a gene transferred 100% of parents to children.
The mode of action of the gene, the factors that affect it and the degradation of scoliosis remain unknown to date and many theories have been developed so far.
Usually there is not a patient whose one or both parents do not have some degree of scoliosis.
The mode of action of the gene, the factors that affect it and the deterioration remain unknown at this time.
With many theories having been developed so far, such as hormonal abnormalities, asymmetric growth and loss of muscle balance.

A genetic test, called ScoliScore., Is available as an adjunct to clinical and radiographic information to determine the risk of developing Adolescent Scoliosis.
How do we understand Adolescent Scoliosis?
Observation
We observe the child visually and identify the following:


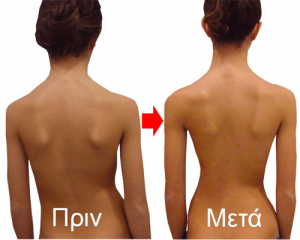
1. Thoracic hump. A wide protrusion on the back or waist is the most visible sign of scoliosis

2. Shoulder height asymmetry and shoulder blades. One shoulder appears higher than the other. The same goes for me shoulder blades

3. Loss of the trunk support. Shifting the body to the right or to the left

4. Pelvic tilt. It appears as an asymmetrical waist in which a hip seems to be higher than the other.

Diagnostic tests
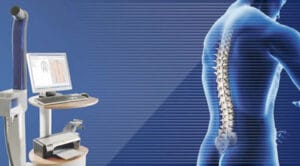
Three-dimensional imaging Formetric 4D
Using Moire principle and after computer processing, without touching the patient, a harmless light and Laser scanner offers us three-dimensional imaging of the Spine with the almost the precision of an X-ray.


It measures the angle of the humps with greater precision as it concerns scoliosis and the kyphotic hump of the kyphosis, not statically, like the simple scoliometer, but dynamically with a hump average value.


X-rays
Full body digital x-rays of low radiation.
They should be done if the previous methods showed mild to moderate scoliosis.
In these we accurately measure the Cobb angle, ie the angle of inclination of the scoliosis.
We also see the Riser point, ie the adolescent’s developmental expectation.


How is it treated?
Adolescent Scoliosis at the beginning of their appearance and up to 25 ° have elastic properties that return to normal levels after appropriate treatment.
Growing up, however, the inclination angle and passing enough time from their appearance, create permanent plastic deformations of the vertebrae resulting in the inability to restore even with appropriate treatment.
That may revert the angle tilt and shift but not the deformation of the vertebrae which means the patient should be continued maintenance of the result.
So in all scoliosis we should intervene very early and effective before creating irreversible damage.

Monitoring is performed in patients whose scoliotic angles are less than 12º.
It is essentially the patient’s re-examination by the attending physician. The examination should include:
- Visual examination,
- examination with electronic or conventional scoliometer (if the data have been recorded in the previous examination),
- check with three-dimensional imaging Formetric 4D (it has a program for comparing previous tests, identifying differences and possible deterioration).
If there is a significant worsening of scoliosis then the patient should undergo X-rays.
Monitoring should not be done at regular intervals, which is unfortunately common, as the adolescent may not have entered a phase of rapid development.
The ideal is to monitor each increase in height of 4-5 cm. So parents should check the height at regular intervals.
Scoliosis in adolescents. Treatment

Progression of scoliosis
The deterioration of scoliosis is unpredictable.
No one can yet say for sure if a 10 ° or 15 ° scoliosis will get worse. There are scoliosis that do not grow much and remain low for the start of a treatment. Most scoliosis statistically, however, deteriorate unpredictably.
Trangenomic, a US company, has developed a genetic test called SCOLISCORE, which predicts a possible worsening of scoliosis in a child.

Unfortunately, its mediocre results in predicting deterioration and its high price ($ 2,800) make it almost prohibitive for widespread use.
If the adolescent is in the phase of rapid growth (> 10 cm per year) usually one year before and one year after the onset of menstruation, scoliosis can worsen greatly. Up to 15 degrees in 6 months.
The treatment of adolescent scoliosis with all-day application of the brace should be applied until the epiphyses are closed, ie until the certified end of bone development (this is practically estimated at about 2 to 4 years from the beginning of the period in girls).
The reason is as shown by the following example that there is a percentage loss of correction if there is still growth, regardless of age.
Example
Patient aged 16 years with left thoracic lumbar scoliosis 32.7 ° and Riser grade 3.
She was applied to SPONDYLOS brace Rigo Cheneau and trained in exercise programs.
The patient applies the brace 21 hours a day.
Two years later her scoliosis had been corrected by 63%, reaching 13.8 ° without a brace.
Although the patient was 18 years old, the growth rate was Riser 3 to 4.
She then decided not to apply the brace and not to exercise, considering that due to his age he had finished the treatment of scoliosis.
The result was that one year later the angle of its scoliosis had increased to 17.8 ° and two years later it had reached 20.2 ° and its epiphyses were still slightly open.

Initial: 32°

After 2 years: 13°

After 3 years: 18°

After 4 years: 20°
After bone maturation, the patient should exercise daily with the exercises has learned and immediately after the end of the exercises to apply the brace for about 8 hours (maybe during sleep).
This is from 6 to 12 months depending on the case.
![]() The treatment of adolescent scoliosis is a constant battle throughout the patient’s life.
The treatment of adolescent scoliosis is a constant battle throughout the patient’s life.
Finishing with the brace application, you should exercise daily for at least 4 years in all exercise programs.
In adulthood you should practice daily for 10 to 15 minutes in specific exercises that will be indicated.
Also in future pregnancies should not take a lot of weight and postpartum
should follow the exercise program for at least six months.
.
Surgical Treatment
Surgical treatment should be applied according to the following indications:
1- Large angles> 65 ° – 70 ° combined with hypokyphosis <10 ° and vital capacity in the lungs <40%
2- Particularly large aesthetic problem, which could not or was not even attempted to be corrected

As a rule, of course, in all specialties of surgery, we must always, before proceeding to a surgical treatment, have exhausted all the possibilities provided by a properly applied conservative treatment.
There is no preventive surgical treatment for scoliosis. We do not operate on a scoliosis because the child will become more beautiful, nor as a precaution so that he does not have a cardiorespiratory problem when he grows up.