SPONDYLOS menu →









Unfortunately, conservative treatment must be carried out at an age which is difficult and very emotionally stressful for the child, usually a girl.
It is a period when the child is beginning to form its sexual identity, and thus reacts to any effort of wearing the brace.
In one of our papers, which was presented at the international conference of the scientific company for the treatment of the Spine Conditions SOSORT, in Montreal in 2010, the reasons why a child does not wear his brace were investigated.
The results were impressive because the children did not have a problem with the brace at home, with his parents and relatives, but they had a problem at school.
This demonstrates the need for children so that their appearance is not affected by the application of the brace.
The downside is that it is this age that is crucial for the correction of scoliosis. As ell as for its deterioration.
Surgery or conservative treatment?

This is a question that has been concerning physicians and patients for 40 years.
We must not condemn either option, as both have their indications, which, however, change over the years.
As a rule, of course, that exists in all surgical specializations, before we proceed with surgery, we must exhaust all other possibilities that a correctly applied conservative treatment provides.
There is no preventive surgical treatment for scoliosis, as I have many times heard from colleagues. We do not operate on a scoliosis to make a child more attractive, nor do we perform surgery preventively so that the child does not have a cardio-respiratory problem when it is older.
But let us see certain myths on the surgical treatment of Scoliosis.
1. Scoliosis will create a major cardio-respiratory issue.
There are few cases of adolescent idiopathic scoliosis that reach the stage of an intense respiratory problem with a reduction in vital capacity and FVC1 of less than 30%. Patients with neuromuscular scoliosis are more affected with other concomitant problems, which affect, among others, the cardio-respiratory system. These patients usually move with the aid of a wheelchair and necessary help from their parents.


Adolescent Scoliosis 138°

with Hypokyphosis 2°

90° neuromuscular scoliosis, resulting

from spinal muscular atrophy.
The respiratory capability is affected in large scoliosis of > 70° with a rotation of > 24° and hypokyphosis of < 11°*
*** Relation between the Characteristics of A.I.S. and Vital Capacity in young and adults D. Papadopoulos, M. Kapetanakis, SOSORT Congress Montreal, May,20-22,2010
There are large scoliosis where the respiratory capability of the patient is not gravely affected due to their athletic activity.
As far as heart problems are concerned, these are concomitant anomalies on the grounds of Idiopathic Scoliosis and not problems that are created by the Scoliosis * **.
*** The findings of preoperative cardiac screening studies in adolescent idiopathic scoliosis. Ipp L, Flynn P, Blanco J, Green D, Boachie-Adjei O, Kozich J, Chan G, Denneen J, Widmann R. J Pediatr Orthop 2011 Oct-Nov;31(7):764-6.
*** Prevalence of cardiac dysfunction and abnormalities in patients with adolescent idiopathic scoliosis requiring surgery. Liu L, Xiu P, Li Q, Song Y, Chen R, Zhou C. Orthopedics 2010 Dec 1;33(12):882.
2- Scoliosis will create a neurological problem in the lower limbs
Only during the surgical correction of a large scoliosis, can a neurological problem be created in the lower limbs, rather than by the scoliosis in itself.
International bibliography has not reported such a case of a neurological problem.
3. Με το χειρουργείο σκολίωσης θα αποφύγουμε τους πόνους.
This is another myth.
If we do not perform spinal fusion all the way to the last vertebra, that is down to the sacral spine, the discs of the free vertebrae L4-L5 and L5-S1 will soon be damaged due to the fact that they are subjected to the larger stresses than the normal, which results in the development of hernias and degeneration. Also, post-operative pain is one of the most common complications of surgery, and it often lasts for a long time.
4- Today there are no specific complications from the operation
Indeed complications today are less than 30 years ago; however, they exist.
Major complications:
- Death < 1%
- Pseudoarthrosis ~5%
- Invasive infection ~3,1%
- Neurological complications ~1,5% (paraplegia, paresis, peripheral neurological damage)
- Delayed bacterial infections ~2,9%
- Wrong positioning of the screws ~15.8 %
Minor complications :
- Asymptomatic failure of materials
- Protrusion of the rods, forcing re-operation and removal of materials
- Spondyloarthritis
- Post-operative pain
- Progressive worsening of the curve
- Increase of the hump
- Susceptibility to spine fractures following accidents
- Stiffness and loss of spine biomechanics

*** Rate_of_complications_in_scoliosis_surgery1 Hans-Rudolf Weiss and Deborah Goodall, Scoliosis 2008, 3:9
Loss of the initial correction and aggravation of the angle

1997 44°

1998 41°

2001 54°

2012 54°
Material failure and loss of correction with concomitant protrusion of rods through the surface of the body




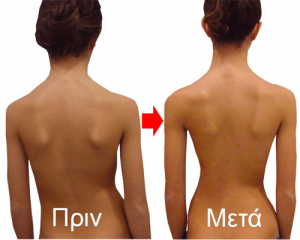
5. Surgery will restore symmetry in the body and humps will disappear.
This is a myth.
In a large Scoliosis, even after a successful spinal fusion without complications, the angle cannot be reduced by more than half, and the humps are usually minimally decreased. Symmetry is not restored, because the center of balance in the brain will create counteraction in the sections outside the fusion in the shoulders and the pelvis.





